
こんにちは。
アトピー研究家の齋藤です。
アトピーは日本特有の病気ではありません。
アメリカでもアトピーを発症する方はたくさんいます。
このページでは「アメリカの州別アトピー有病率」のデータをご紹介致します。
アメリカの州別アトピー有病率
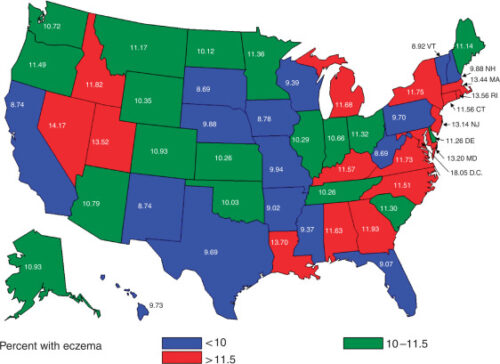
アメリカの州別アトピー有病率は、下記のグラフと表をご覧下さい。
表は6までありますが、この記事では表1と表2を引用しています。
詳しく知りたい方は、引用元をご確認下さい。
なお、アメリカでは「atopy」という言葉は一般的ではなく、「eczema」(湿疹)という言葉が使われています。
そのため、「eczema」を「アトピー」として日本語訳をしています。
引用サイトは下記になります。
https://www.jidonline.org/article/S0022-202X(15)35013-2/fulltext
Overall, a total of 9,752 children had a diagnosis of eczema, which translated to a 10.7% national prevalence of eczema in children under 18 years of age. The disease prevalence ranged from 8.7 to 18.1% between states and districts. Figure 1 and Table 1 present state prevalence estimates for US children (0–17 years of age), who were reported to have a diagnosis of eczema in the past 12 months. The highest state prevalence values were reported in many East Coast states, as well as in Utah, Idaho, and Nevada. The lowest state prevalence values were in the middle and southwestern parts of the country (Table 1).
Journal of Investigative Dermatology 131, 67 (2010). doi:10.1038/jid.2010.251
Table 1
Eczema prevalence by state(アメリカの州別アトピー発症率)
| State/district | Frequency | Percentage | 95% Confidence interval |
| West Virginia | 159 | 8.100 | (7.21, 10.18) |
| South Dakota | 136 | 8.100 | (6.93, 10.46) |
| California | 180 | 8.74 | (7.26, 10.22) |
| New Mexico | 142 | 8.74 | (7.08, 10.39) |
| Iowa | 159 | 8.78 | (7.27, 10.30) |
| Vermont | 154 | 8.92 | (7.30, 10.54) |
| Arkansas | 139 | 9.02 | (7.31, 10.73) |
| Florida | 159 | 9.07 | (7.34, 10.80) |
| Mississippi | 147 | 9.37 | (7.56, 11.19) |
| Wisconsin | 162 | 9.39 | (7.78, 11.00) |
| Texas | 174 | 9.100 | (8.08, 11.30) |
| Pennsylvania | 200 | 9.7 | (8.18, 11.23) |
| Hawaii | 173 | 9.73 | (8.04, 11.43) |
| Nebraska | 147 | 9.88 | (8.09, 11.66) |
| New Hampshire | 179 | 9.88 | (8.35, 11.41) |
| Missouri | 189 | 9.94 | (8.36, 11.52) |
| Oklahoma | 165 | 10.03 | (8.36, 11.71) |
| North Dakota | 154 | 10.12 | (8.31, 11.93) |
| Tennessee | 176 | 10.26 | (8.49, 12.03) |
| Kansas | 156 | 10.26 | (8.40, 12.11) |
| Illinois | 203 | 10.29 | (8.61, 11.98) |
| Wyoming | 168 | 10.35 | (8.67, 12.02) |
| Indiana | 164 | 10.66 | (8.84, 12.48) |
| Washington | 190 | 10.72 | (9.07, 12.37) |
| Arizona | 152 | 10.79 | (8.86, 12.71) |
| Alaska | 165 | 10.93 | (9.08, 12.78) |
| Colorado | 194 | 10.93 | (9.21, 12.65) |
| Maine | 187 | 11.14 | (9.36, 12.92) |
| Montana | 185 | 11.17 | (9.38, 12.96) |
| Delaware | 228 | 11.26 | (9.67, 12.86) |
| South Carolina | 208 | 11.3 | (9.100, 13.00) |
| Ohio | 220 | 11.32 | (9.66, 12.97) |
| Minnesota | 168 | 11.36 | (9.39, 13.32) |
| Oregon | 188 | 11.49 | (9.100, 13.29) |
| North Carolina | 204 | 11.51 | (9.75, 13.27) |
| Connecticut | 241 | 11.56 | (9.93, 13.20) |
| Kentucky | 204 | 11.57 | (9.80, 13.33) |
| Alabama | 216 | 11.63 | (9.84, 13.41) |
| Michigan | 222 | 11.68 | (9.98, 13.39) |
| Virginia | 220 | 11.73 | (9.97, 13.49) |
| New York | 222 | 11.75 | (10.01, 13.49) |
| Idaho | 1100 | 11.82 | (9.93, 13.71) |
| Georgia | 192 | 11.93 | (10.00, 13.86) |
| New Jersey | 270 | 13.14 | (11.36, 14.91) |
| Maryland | 261 | 13.2 | (11.37, 15.03) |
| Massachusetts | 265 | 13.44 | (11.65, 15.23) |
| Utah | 1100 | 13.52 | (11.39, 15.65) |
| Rhode Island | 258 | 13.56 | (11.68, 15.45) |
| Louisiana | 2100 | 13.7 | (11.74, 15.66) |
Of those children with eczema, 30.7% reported concurrent hay fever and 22.8% reported concurrent asthma consistent with similar AD populations in Europe (Asher et al., 2006; Van der Hulst et al., 2007). As expected, age of the child was a significant determinant of eczema prevalence, given the natural course of the disease (Table 2 ). There was a significant effect of the highest reported education level in the household on eczema prevalence, with those households reporting education levels greater than high school having the greatest prevalence of eczema (Table 2). Other significant demographic variables showing positive associations with disease prevalence included living in a metropolitan area (defined using RUCA (Rural-Urban Commuting Area) codes), speaking English as the primary language, and being of Black or multiple race (Table 2).
Table 2
Eczema prevalence stratified by primary demographic variables
(アトピーの発症率:主要な人口構成)
| Variable | Subgroup | Frequency | Percentage | 95% Confidence interval | P-value |
| Age | <4 years | 2,977 | 13.92 | (13.12, 14.73) | <0.0001 |
| 4–8 years | 2,623 | 10.63 | (9.98, 11.27) | ||
| 9–12 years | 1,862 | 9.96 | (9.23, 10.68) | ||
| 13–17 years | 2,290 | 8.56 | (7.97, 9.16) | ||
| Gender | Male | 4,874 | 10.52 | (10.04, 11.01) | 0.3507 |
| Female | 4,867 | 10.85 | (10.36, 11.34) | ||
| Highest education level completed by parent | <HS | 278 | 6.95 | (5.63, 8.27) | <0.0001 |
| HS | 1,721 | 9.61 | (8.89, 10.33) | ||
| >HS | 7,721 | 11.47 | (11.06, 11.88) | ||
| Residence in metropolitan area | No | 1,442 | 8.53 | (7.90, 9.16) | <0.0001 |
| Yes | 5,161 | 10.99 | (10.55, 11.43) | ||
| Primary language spoken at home | English | 9,273 | 11.15 | (10.78, 11.51) | <0.0001 |
| Any other | 474 | 6.91 | (5.89, 7.94) | ||
| Race | White only | 6,770 | 9.7 | (9.34, 10.05) | <0.0001 |
| Black only | 1,464 | 15.89 | (14.64, 17.14) | ||
| Multiple race | 550 | 15.03 | (12.97, 17.10) | ||
| Other | 470 | 10.08 | (8.36, 11.80) | ||
| Household income | 0–99% FPL | 1,037 | 10.38 | (9.40, 11.37) | 0.0357 |
| 100–199% FPL | 1,732 | 11.09 | (10.18, 12.00) | ||
| 200–399% FPL | 3,135 | 10.21 | (9.65, 10.77) | ||
| ≥400% FPL | 3,024 | 11.53 | (10.91, 12.15) |
今回引用したデータについて
Using the 2003 National Survey of Children’s Health sponsored by the federal Maternal and Child Health Bureau, we calculated prevalence estimates of eczema nationally and for each state among a nationally representative sample of 102,353 children 17 years of age and under. Our objective was to determine the national prevalence of eczema/atopic dermatitis in the US pediatric population and to further examine geographic and demographic associations previously reported in other countries. Overall, 10.7% of children were reported to have a diagnosis of eczema in the past 12 months. Prevalence ranged from 8.7 to 18.1% between states and districts, with the highest prevalence reported in many of the East Coast states, as well as in Nevada, Utah, and Idaho. After adjusting for confounders, metropolitan living was found to be a significant factor in predicting a higher disease prevalence with an odds ratio of 1.67 (95% confidence interval of 1.19–2.35, P=0.008). Black race (odds ratio 1.70, P=0.005) and education level in the household greater than high school (odds ratio 1.61, P=0.004) were also significantly associated with a higher prevalence of eczema. The wide range of prevalence suggests that social or environmental factors may influence disease expression.
補足説明
この記事で引用したデータは、2003年のデータになりますので、約20年前のデータになります。
ただ、先進国の場合は、現在でも、ほとんど変わっていないと考えられます。
その理由は、環境があまり変わっていないからです。
私はアメリカを何度も訪れていますが、20年前と現在では大きな違いはありません。
これは、日本も同じです。
逆に、今後、アトピーの患者が増えていく国は、中国、フィリピン、ベトナム、タイなど、どんどんと経済発展していく国になると思います。
経済的に豊かになると、生活環境がどんどんと変わってくるからです。
まとめると、先進国のアトピーのデータに関しては、2000年以降は大きな変化は少なく、発展途上国のデータに関しては、今後、発症率が増えていく可能性が高いのです。
コメント